Moving from Zepbound to Wegovy isn't as simple as swapping one pen for another. Honestly, it's more like trying to translate a poem from one language to another—you can get the gist right, but the nuances are where things usually get messy.
In early 2026, we’re seeing a massive wave of people making this switch. Why? Mostly because insurance formularies—looking at you, CVS Caremark—have been dropping Zepbound like a hot potato in favor of Wegovy. It’s rarely about which drug works "better" for your body and almost always about which one the bean counters at the insurance company got a better deal on.
But if you're the one holding the needle, those corporate deals don't matter. What matters is not spending your weekend huddled on the bathroom floor because your dose was miscalculated.
The "Equivalent" Dose Myth
Here is the cold, hard truth: there is no official, FDA-sanctioned conversion chart for zepbound to wegovy conversion.
None.
The two drugs aren't even the same type of medicine. Wegovy (semaglutide) is a GLP-1 receptor agonist. Zepbound (tirzepatide) is a "dual agonist," hitting both GLP-1 and GIP receptors. Because Zepbound works on two pathways, it’s generally more "potent" pound-for-pound in clinical trials.
If you were on the max dose of Zepbound (15 mg), you might think you should jump straight to the max dose of Wegovy (2.4 mg).
Don't do that.
Even if you’ve been on Zepbound for a year, your body isn't used to the specific way Wegovy hits those GLP-1 receptors. Doctors like Dr. Scott Isaacs and other obesity medicine specialists often warn that "switching across" at high doses is a recipe for severe nausea and vomiting.
What the typical transition looks like
Most clinicians follow a "reset" or "step-down" strategy. It feels like a setback, but it's actually just safety.
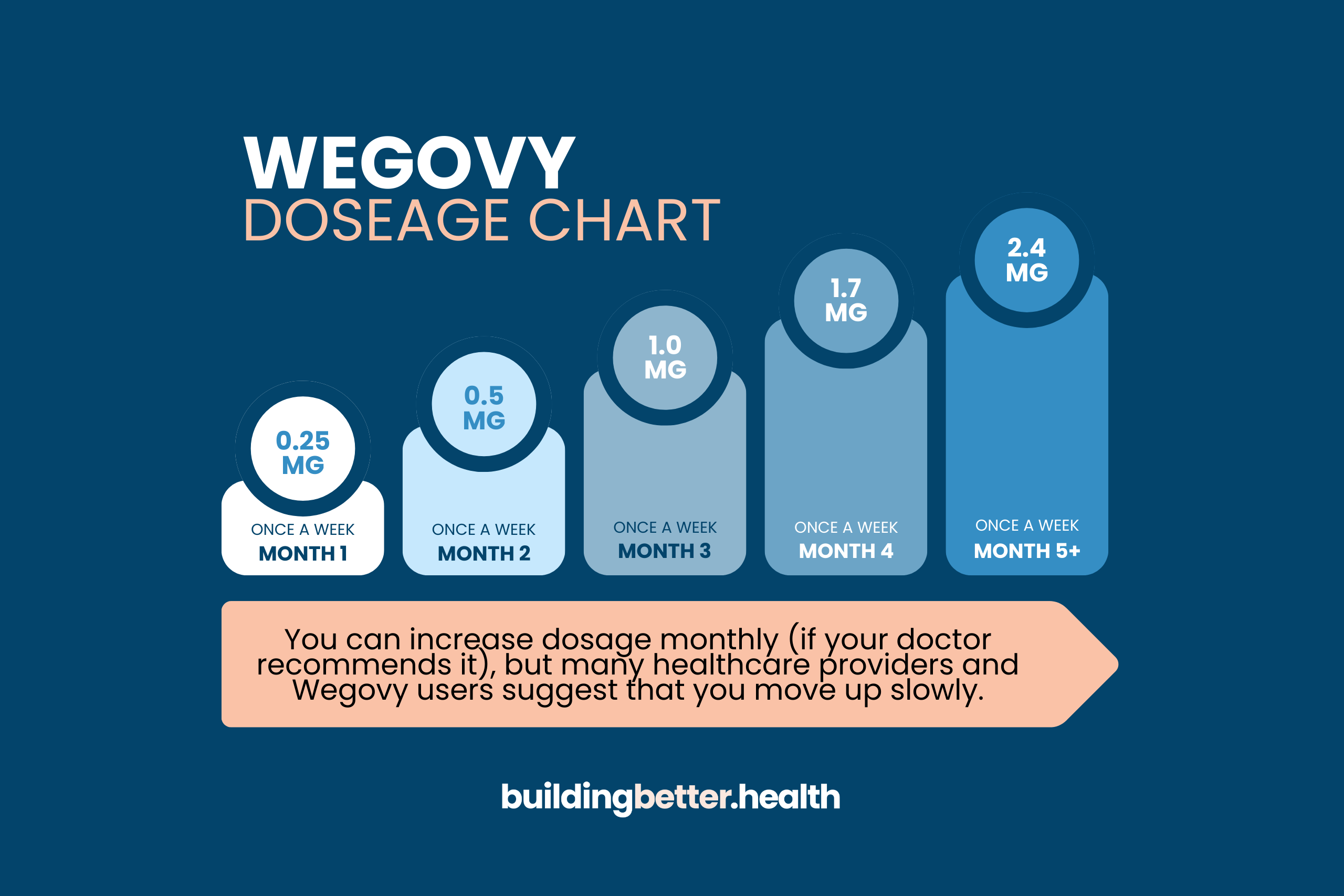
- If you were on Zepbound 2.5 mg or 5 mg: Most doctors start you at the beginning of the Wegovy ladder—0.25 mg or 0.5 mg.
- If you were on Zepbound 7.5 mg or 10 mg: You might start at Wegovy 1.0 mg.
- If you were on the heavy hitters (12.5 mg or 15 mg): Some brave souls try to start at Wegovy 1.7 mg, but many doctors still insist on starting at 1.0 mg to see how you handle the different chemical profile.
Why the GIP Factor Changes Everything
Zepbound’s "GIP" component is sort of like a buffer. It helps with insulin secretion but also seems to mitigate some of the nausea that comes from the GLP-1 side. Wegovy doesn't have that buffer.
When you lose the GIP component, your body is suddenly dealing with a "pure" GLP-1. You might find that even though Wegovy is technically "weaker" in terms of total weight loss percentage in studies (averaging around 15% vs Zepbound’s 21%), the side effects feel "sharper."
It’s weird. You’d think moving to a less potent drug would be easier. Often, it’s the opposite.
The Logistics of the Switch
You don't need a "washout" period. You don't need to wait three weeks for the Zepbound to leave your system.
The standard protocol is simple: take your last dose of Zepbound, wait seven days, and then take your first dose of Wegovy on your usual "shot day."
If you’re switching because of a shortage—which, let's be real, is still happening in 2026—and you’ve already been off Zepbound for more than two weeks, your doctor will almost certainly make you start Wegovy at the absolute bottom dose (0.25 mg). Your tolerance for these drugs disappears surprisingly fast.
The "Plateau" Anxiety
Let's talk about the elephant in the room. Are you going to gain weight?
Maybe a little. Or you might just stall.
When you perform a zepbound to wegovy conversion, you are moving from a dual-hormone drug to a single-hormone drug. Clinical data from the SURMOUNT and STEP trials consistently show Zepbound has a slight edge in raw weight loss numbers.
If you move from 15 mg of Zepbound down to 1.0 mg of Wegovy to stay safe, your appetite might come roaring back for a few weeks. That’s not the drug "failing." It’s just the titration process. You have to climb the Wegovy mountain from the bottom, even if you already summited the Zepbound one.
Real-world expectations
- The First Month: Expect to feel "more hungry" than you did on Zepbound. This is normal.
- The Side Effect Shift: You might trade Zepbound's injection site rashes for Wegovy's notorious "sulfur burps" or constipation.
- The Long Game: Once you hit the 2.4 mg maintenance dose of Wegovy, most people find they can maintain their Zepbound losses, even if the "active" losing phase slows down.
Insurance and the "Prior Auth" Nightmare
Even though Zepbound and Wegovy are both for obesity, your insurance company treats them like totally different categories.
Just because you had a Prior Authorization (PA) for Zepbound doesn't mean it magically carries over to Wegovy. However, in 2026, many PBMs have started "fast-tracking" these switches because they want you on the cheaper drug.
If your doctor writes the script for the switch, make sure they note "medication transition due to formulary change." This usually triggers a faster approval than a brand-new "starting" request.
Actionable Steps for a Painless Switch
If you're staring at a new box of Wegovy and a half-empty box of Zepbound, here is how you handle it like a pro:
- Ask for Zofran: Before you take that first Wegovy shot, have a prescription for Ondansetron (Zofran) ready. You might not need it, but if the "pure" GLP-1 hits your stomach hard, you'll be glad you have it.
- Hydrate Like It's Your Job: Electrolytes matter more during a switch. Your GI tract is about to go through a transition period, and dehydration makes nausea 10x worse.
- Don't Rush the Titration: If your doctor says stay on 0.5 mg for a month, stay on 0.5 mg. Trying to "catch up" to your old Zepbound strength too fast is the leading cause of ER visits for these meds.
- Track Your "Food Noise": Keep a simple note on your phone. If the food noise is unbearable after the switch, it's a sign your Wegovy dose is too low, and you should advocate for a faster (but safe) move up the ladder.
The transition is a marathon, not a sprint. You've already done the hard work of starting the journey; this is just a detour in the road. Keep your eye on the maintenance goal and give your body the grace to figure out a new chemical balance.